A large majority of infertile population goes untreated due to several possible reasons. An insight by Dr Chetana V, Bmom, Bangalore
Infertility rates are on the rise due to a variety of risk factors such as lifestyle, food habits, late marriage, stress and other environmental factors. As per WHO estimates, infertility rates are observed to be increasing in urban
areas wherein one in six couples are impacted. Infertility incurs negative socio-economic impacts on the lives
of the infertile couple and particularly women who frequently experience violence, divorce, personal trauma,
anxiety, social stigma and low self esteem due to their inability to conceive a child. Thus, in a nutshell, IVF clinics play a crucial role in providing effective treatment services to achieve minimised time for conception possibilities.
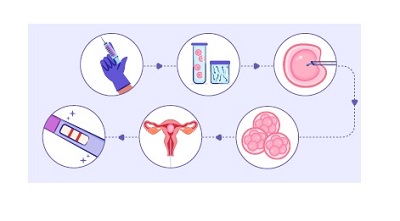
The first step at Bmom for any couple that visits us for assistance is to find out if there are any known issues in
male and/or female gametes (egg and sperm). The next step is to take them through natural or IUI procedures for conception. These are considered noninvasive and a couple can go for three to five times or more if no known cause is found in the preliminary screening and diagnostic tests.
Patients, with known causes or for those the above treatments have not brought out the likely outcome, are counselled for the IVF treatment explaining about the procedure and what to expect. Once patients are mentally prepared for the treatment, several consent documents are signed to initiate the treatment. Controlled hyperstimulation (aiming at 10 good responsive follicles) is started followed by induction of ovulation. While these steps might indicate where the problem might have occurred, the true indication of the actual quality of gametes would come when IVF/ICSI is performed. The first concern is to have a good number of follicles which house the egg. Many times follicle is considered a synonym for egg but in reality that is not the case. Having a good number of follicles that also have a good number of eggs is imperative for IVF/ICSI. Once the eggs are aspirated out of follicles we can have a visual confirmation under a microscope (as they are less than 10th of a millimetre) as to the quality of the eggs. It is important to have quality and not only quantity when it comes to eggs. When it comes to sperm processing, cryopreservation and IMSI are some of the techniques that will help choose the best sperm. Once the best possible eggs and sperms are chosen IVF/ICSI is performed which would yield embryos (the number of formed good quality embryos relies on the fate of developmental potentials) that would hopefully yield in a successful conception after transfer to the uterus. More good-quality embryos mean the possibility for multiple transfers if the first trial fails. Whereas, suboptimal quality embryos reflect the stress in a lower success rate.
If the sperm or eggs are suboptimal or of poor quality, there are treatment options to improve the quality. There is also the option of donor sperm or oocyte or donor embryo programs that help the couple to achieve embryo transfer into the uterus and then wait for implantation and BFP (Big fat positive) with UPT or good beta HCG. The true confirmation though would be to do an ultrasound for a foetal heartbeat. Even though one opts for IVF, it is
stressful to wait to know if everything is going fine and further waiting period after embryo transfer for a positive result. Despite all the precautions and confirmations, a positive outcome is not guaranteed. The worse will be to cope with the negative result or to lose it (for some reason) midway and to gather the courage to tackle it all over again. It is pretty stressful, desperate and nerveshattering. Toughest would be to deal with repetitive implantation failure.
The average IVF success rate worldwide using own oocytes and sperm falls between 20-40 per cent and donor
options would raise the hope to 50-80 per cent when the embryos make it to day 5/6 of their developmental stage. But, the majority of the times time sperm, egg or embryo quality either may be a self-cycle or and donor cycle that hinder the success of IVF.
IVF treatment does not improve the quality of oocytes in the ongoing cycle but rather selects the best ones, but, perhaps it removes the poor-quality oocytes from the ovary, there might be hope for better quality egg formation in the next cycles. For example, IVF cycles failure and/or RIF would conceive naturally after a few months or years, once the couple is given up on IVF treatment due to lost hope, tiered or money factor but question is how many couples do conceive after giving up the treatment is an important consideration before thinking about the reason of IVF failures.
Currently in India, 2-3 lakh IVF cycles are performed to treat infertility, which accounts for about only 10 per cent of the total infertile population. Thus, a large majority of the infertile population goes untreated due to several possible reasons such as lack of awareness, affordability and apprehensions. Prospective couples reaching out
to the clinic are supported with the complete journey and their odds of each step prepare them for the assisted reproduction procedure with the help of infertility specialists as described in. During IVF treatment, we have observed that the patient who is undergoing ART, approximately around 15 per cent of patients get conceived in the first line of treatment which is IUI with an MC rate observed to be around 18 per cent. By the time hope of IUI positive moved to IVF interventions inevitably fall around 33-34 years of average age. As per our observation from unbiased cumulative data, the age under 38 years did not impact the success rates. on the other hand, we have observed an interesting trend in miscarriages post embryos transfer (IVF) seems to be around 9 per cent, but a significant increase was observed in 2019 and 2020, which might not exclude the covid impact on
miss carriages as well other inherent clinical factors. Over the last four years, during the time of our observation, it appears that, at our clinic, success rates using self-gametes were 40 per cent whereas, improvising the treatment options with donor gametes improved to 60 per cent which may provide a hint that the couple undergoing IVF treatment at the age of 35 years shows the sign of compromised gamete quality over the endometrium implantation function.
Moreover, we have observed that an avg blastocyst formation rates are near 40 per cent to a maximum of 50 per cent under optimal gamete quality independent of age. The morphological parameters of D5/6 blastocysts that gave us live births showed varying morphological features, yet observed healthy live.
A trend towards having more blastocysts has seen a positive outcome over the morphological parameters of d5/d6 embryos. Hope that our observations and data and scientific representation from a single centre might provide hints in routine IVF treatment options and success rate improvement. In addition to our implementation of
the procedure in each step, we vest our efforts in improving overall success rates per IVF by working in technologies that provide objective and productive parameters as described in. We work closely with our academic and industrial partners in advanced technologies in the areas of sperm selection, oocyte quality understanding and embryo selection methods using artificial intelligence.
Moreover, we utilise our motivation to be ARTists (Assisted Reproductive Technologists), learning skills from the
clinical and scientific side to fill the gaps in digital medicine and engineering team to contribute our part to building better systems and technologies for the best possible results and patient care.



